

Background: Allogeneic hematopoietic transplantation (HCT) is frequently considered for patients (pts) with relapsed T-cell lymphoma (TCL) and less often as consolidation of initial therapy. Outcomes from prior registry data show that only 31% of pts remain disease free 3 years after HCT (Smith et al. JCO 2013). However, several single institution studies have superior outcomes. We previously presented an analysis of allogeneic transplant in T-cell lymphoma but have expanded this effort to 12 academic centers with longer follow up (Mehta-Shah ASH 2017).
Methods: We analyzed the patient characteristics at time of diagnosis and transplant, treatment history, overall (OS) and progression-free survival (PFS) in consecutive TCL pts who had an HCT from 1/1/2000-12/31/2019 at 12 academic institutions.
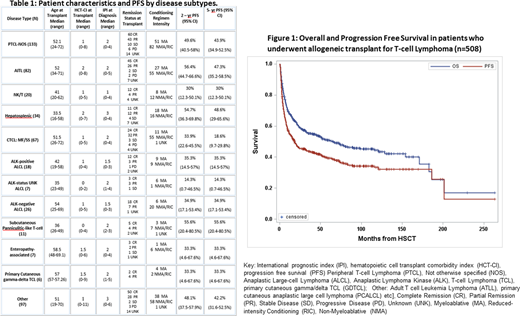
Results: Patient characteristics are shown in Table 1. 508 pts were identified with median age 51 years (16 - 72). 452 (86.5%) had known remission status at the time of HCT: 245 (54.4%) complete remission (CR), 168 (37.2%) partial remission (PR), 23 (5.0%) stable disease (SD), 16 (3.2%) progressive disease (PD). Seventy-eight (15.5%) had a prior autologous HCT. Thirty-six (7%) pts underwent HCT in CR1, 352 (69%) for relapsed/refractory TCL, and was not specified in 120 pts (24%). The median HCT comorbidity index (HCT-CI) score was 1 (0-11).
Conditioning regimens were myeloablative (n=180), reduced intensity/non-myeloablative (n=323), unknown (n=3). Donor type was known for 471 pts: 192 matched related (MRD), 183 matched unrelated (MUD), 53 mismatched (MMD), 18 haploidentical donors, 25 umbilical cord blood.
In this series, the 2 year OS and PFS rate following HCT were 59.1% (95%CI: 54.6-63.3%) and 45.8% (95%CI: 41.3-50.2%) respectively. 5 year OS and PFS rate were 50.8% (95%CI: 46.1-55.3%) and 39.4% (95%CI: 34.9-43.9%) (Fig 1) For disease specific 2-year and 5-year PFS, see Table 1. At a median follow-up of 29.7 mo (0.1-263 mo), 163 pts had relapsed and 261 pts had died. The median time from relapse post HCT to death was 10.2 mo (0-158.4 mo). Of 261 deaths: 81 were due to transplant related mortality (TRM), 69 were confirmed to be from TCL, and 111 were from non-relapse mortality/unknown. There was not a significant difference in PFS for pts with AITL, PTCL-NOS, ALK positive ALCL or ALK negative ALCL, with median PFS of 23.2 mo (95%CI:15.3-64.2). However, when AITL was compared specifically to PTCL-NOS or ALCL, those with AITL had a trend towards improved median PFS (51.4 mo vs. 18.4 mo, p=0.14) and improved median OS (not reached vs. 73.1 mo, p=0.26). At 5 years, PFS was worse for CTCL (18.6%, 95% CI: 9.7%-30.0%) compared to PTCL subtypes (43.8%; 95% CI: 37.3%-50.0%)(p<0.001) . However, 5-year OS was similar for CTCL (44.0%, 95% CI: 30.1-56.4%) and PTCL (53.1%, 95% CI: 46.5-59.3%) (p=0.46). The rate of TRM at 1 year was 11.2% (95%CI:8.5%-14.0%). Of evaluable pts, 245/489 (46%) had acute GvHD and 192/473 (40.6%) had chronic GvHD. There were no differences in TRM according to recipient age (p=0.47). Higher HCT-CI was associated with an increased risk of TRM (HR 1.15, 95% CI: 1.031-1.286; p=0.012)
Disease status at the time of HCT was associated with PFS (p<0.001). Median PFS for those with CR (n=239), PR (n=164), SD (n=22) or PD (n=14) were 44.6 mo, 8.6 mo, 21 mo, 3.5 mo respectively. Degree of donor match was associated with cumulative TRM (p=0.0241). For pts who underwent MRD, MUD, or MMD HCT, cumulative TRM at 12 months was 8% (95%CI: 5.5-12.2%), 13.1% (95%CI: 9.7-17.8%), 14.7% (95%CI: 8.7-24.6%).
Conclusions: We present the largest series of HCT in TCL. In this dataset, HCT provided durable disease control for a significant portion of pts with relapsed or refractory or otherwise high risk TCL. Depth of response to therapy immediate prior to HCT was associated with PFS. Patients with AITL appeared to have a trend towards improved outcome with HCT compared to other common PTCL histologies. Patients with CTCL had a higher rate of relapse compared to PTCL subtypes, but OS was similar. MRD HCTs were associated with lower TRM. This data supports the curative potential of HCT in a patient group with otherwise poor survival and limited treatment options.
Mehta-Shah:Corvus: Research Funding; Genetech/Roche: Research Funding; Verastem: Research Funding; Karyopharm Therapeutics: Consultancy; Bristol Myers-Squibb: Research Funding; Celgene: Research Funding; C4 Therapeutics: Consultancy; Kyowa Hakko Kirin: Consultancy; Innate Pharmaceuticals: Research Funding. Dahi:Kite: Consultancy. Sauter:Sanofi-Genzyme: Consultancy, Research Funding; Kite - a Gilead Company: Consultancy; Spectrum Pharamaceuticals: Consultancy; Gamida Cell: Consultancy; GSK: Consultancy; Bristol-Myers Squibb: Research Funding; Celgene: Consultancy, Research Funding; Novartis: Consultancy; Genmab: Consultancy; Precision Biosciences: Consultancy, Research Funding; Juno Therapeutics: Consultancy, Research Funding. Moskowitz:Merck: Research Funding; Imbrium Therapeutics, L.P.: Consultancy; Bristol-Myers Squibb: Research Funding; Miragen Therapeutics: Consultancy; Merck: Consultancy; Seattle Genetics: Consultancy; Incyte: Research Funding; Seattle Genetics: Research Funding. Jacobsen:Novartis: Research Funding; Takeda: Honoraria; Pharmacyclics: Research Funding; F. Hoffmann-LaRoche: Research Funding; Astra-Zeneca: Consultancy; Acerta: Consultancy; Merck: Consultancy. William:Celgene: Consultancy, Honoraria; Guidepoint Global: Consultancy; Seattle Genetics: Research Funding; Dova: Research Funding; Incyte: Research Funding; Merck: Research Funding; Kyowa Kirin: Consultancy, Honoraria. Barta:Monsanto: Consultancy; Pfizer: Honoraria; Janssen: Honoraria; Seattle Genetics: Honoraria, Research Funding; Atara: Honoraria. Allen:Clinical Care Options: Speakers Bureau; Curio Sciences: Honoraria; Research to Practice: Speakers Bureau; Imbrium: Consultancy, Other; Bayer: Consultancy, Other. Song:Sanofi: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen, Celgene,Takeda: Consultancy, Honoraria; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees; GlaxoSmithKline: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene/BMS: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria, Research Funding; Otsuka: Honoraria. Ruan:Celgene: Consultancy, Research Funding; Seattle Genetics: Research Funding; Kite Pharma: Consultancy; Juno: Consultancy; BMS: Consultancy, Research Funding; Pharmacyclics: Research Funding; AstraZeneca: Consultancy, Research Funding. McKinney:Kite/Gilead: Honoraria, Speakers Bureau; Kite/Gilead, Seattle Genetics, Molecular Templates, BTG, Pharmacyclics, Verastem, Genentech, Inc., Celgene: Consultancy; UNUM, Molecular Templates, Incyte, Beigene, Denovo Biopharma, Pharmacyclics, Nordic Nanovector, BMS, Genentech, Inc., Celgene: Research Funding. Beaven:Tessa Therapeutics: Research Funding; Roche: Research Funding; Seattle Genetics: Research Funding; MorphoSysAb: Research Funding; LoxoOncology: Research Funding; Celgene: Research Funding. Haverkos:Viracta THerapeutics: Consultancy. Alpdogan:Seattle Genetics: Consultancy; Kiowa Kirin: Consultancy. Porcu:Kiowa Kirin: Research Funding; Kura Oncology: Research Funding; Innate Pharma: Membership on an entity's Board of Directors or advisory committees, Research Funding; Galderma: Research Funding; Daiichi: Consultancy, Honoraria; Celgene: Research Funding; Cell Medica: Research Funding; Miragen: Research Funding; Verastem: Consultancy; Viracta Therapeutics: Membership on an entity's Board of Directors or advisory committees. Horwitz:Daiichi Sankyo: Research Funding; GlaxoSmithKline: Consultancy; Janssen: Consultancy; Kura Oncology: Consultancy; Myeloid Therapeutics: Consultancy; Miragen: Consultancy; ADCT Therapeutics: Consultancy, Research Funding; Aileron: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Forty Seven: Consultancy, Research Funding; Infinity/Verastem: Research Funding; Kyowa Hakka Kirin: Consultancy, Research Funding; Millenium/Takeda: Consultancy, Research Funding; Seattle Genetics: Consultancy, Research Funding; Trillium: Consultancy, Research Funding; Corvus: Consultancy; Innate Pharma: Consultancy; Mundipharma: Consultancy; Portola: Consultancy, Research Funding; Beigene: Consultancy; C4 Therapeutics: Consultancy; Verastem: Consultancy, Research Funding; Vividion Therapeutics: Consultancy; Affirmed: Consultancy; ASTEX: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal